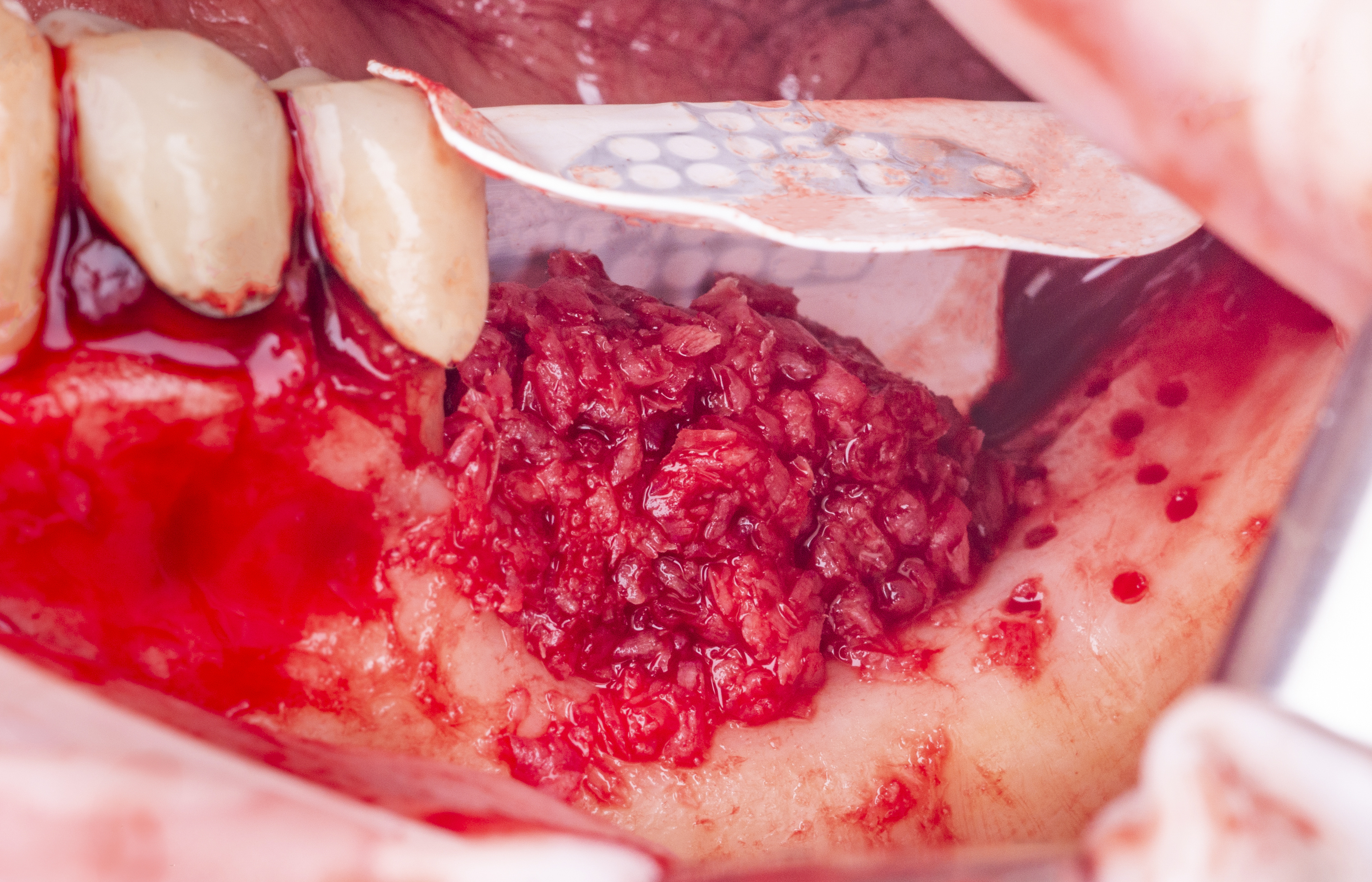
Clinical Case: NeoGen® PTFE Membran
Vertical and horizontal guided bone regeneration
in atrophic posterior mandible using a non-absorbable PTFE membrane with titanium reinforcement.
Dr. Javier Mayor Arenal
Specialist in oral surgery, implantology and periodontics
Madrid, Spain




















